Materials and Methods. We examined 98 patients with CKD in the pre-dialysis period (mean age 47.1±11.2 years). The patients were divided into three groups according to the criteria of CVR stratification. Group 1 consisted of 32 patients with a low or moderate CVR, and CKD stage C1 or C2; Group 2 included 34 patients with a high CVR and CKD stage C3a or C3b; Group 3 comprised 32 patients with a very high CVR and CKD stage C4. We used the SAGE test (Self-Administered Gerocognitive Examination) to evaluate cognitive functions.
Results. Cognitive impairment (CI) was detected in 57% of the patients: 37.5% in Group 1, 44.1% in Group 2, and 90.5% in Group 3. Dementia was diagnosed in 19% of patients with CI. A correlation was found between the severity of CI, the degree of decrease in glomerular filtration rate, and the education level of CKD patients in the pre-dialysis period (p≤0.001). We established that the examined subjects with CKD were characterized by memory, constructive, spatial and logical thinking disorders.
Conclusion. Chronic kidney disease is an independent risk factor for the development of CI. The latter progressed with both CKD stage and the patient’s CVR category, and was detected in 37.5% of patients with a low or moderate CVR, 44.1% of patients with a high CVR, and 90.5% of patients with a very high CVR.
Introduction
Chronic kidney disease (CKD) is among the most wide-spread chronic non-communicable diseases, as well as among the most significant problems of contemporary healthcare. By 2040, CKD is estimated to be the fifth most common cause of reduced life expectancy worldwide [1]. According to the worldwide data, the global prevalence of CKD in the general population averages 14.4% [2, 5], which is comparable to such socially significant diseases as hypertension, coronary heart disease, diabetes mellitus, and obesity [3, 5]. In the Russian Federation, symptoms of CKD are noted in 36% of the population over the age of 60 years, in 16% of people of working age, and in 26% of people with cardiovascular diseases [3, 5].
In the latest revision (2019) of the clinical guidelines by ESC/EAS (European Society of Cardiology / European Atherosclerosis Society) for the correction of dyslipidemia and the reduction of cardiovascular risk (CVR) in clinical practice, the presence of CKD and the level of glomerular filtration rate (GFR) are considered independent criteria determining the patient’s CVR category [4]. Structural and functional pathological rearrangements of the cerebral vascular bed in CKD patients can be explained by the influence of conventional (arterial hypertension, hypercholesterolemia, diabetes mellitus, obesity) and specific (endothelial dysfunction, disorders of phosphorus and calcium metabolism, calcification of the vascular wall and deficiency of the klotho factor, hyperhomocysteinemia, β2-microglobulinemia, accumulation of uremic toxins, anemia, dysfunction of blood cells, oxidative stress, chronic inflammation, etc.) cerebrovascular risk factors [5-7]. It is believed that cerebrovascular diseases among patients with CKD occur at least twice as often as in the general population and potentially determine the cardiovascular prognosis and the risk of developing cognitive impairment (CI) in patients with CKD, both in pre-dialysis and dialysis periods [8-11]. According to a systematic review and meta-analysis by T. Etgen et al. (2012), CKD is an independent somatic risk factor for the development of CI [12].
Objective: to study the cognitive status of patients in the pre-dialysis period depending on the stage of chronic kidney disease and the category of cardiovascular risk.
Materials and Methods
We examined 98 patients with CKD in the pre-dialysis period who were on outpatient treatment from January to November, 2019, at the Urology Center of the Polyclinic No. 3 of the Privolzhsky District Medical Center of the Russian Federal Medical and Biological Agency, and on inpatient treatment at the Nephrology Department at N.A. Semashko Nizhny Novgorod Regional Clinical Hospital. The diagnosis of CKD and CKD stage were identified by a nephrologist in accordance with the Clinical Guidelines of the Association of Russian Nephrologists and with the criteria of the International Classification of Diseases (the 10th revision) (Table 1).
Таble 1. Classification of chronic kidney disease based on glomerular filtration rate values (sensu 2019 Clinical Guidelines of the Association of Russian Nephrologists [3, 5])
|
|
CKD stage (sensu GFR) |
GFR values (mL/min/1.73 m2) |
|
|
Pre-dialysis period of CKD |
С 1 |
High or optimal GFR |
≥90 in the presence of structural or functional kidney damage for ≥3 months |
|
С 2 |
Slightly reduced GFR |
60-89 |
|
|
С 3а |
Moderately reduced GFR |
45-59 |
|
|
С 3b |
Substantially reduced GFR |
30-44 |
|
|
С 4 |
Significantly reduced GFR |
15-29 |
|
|
Dialysis period of CKD (renal replacement therapy) |
С 5 |
End-stage renal failure |
<15 |
CKD – chronic kidney disease; GFR – glomerular filtration rate.
To diagnose and determine the stage of CKD, GFR was calculated using the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) formula, which takes into account race, gender, age, serum creatinine, and is considered the most accurate for adult population [13].
The inclusion of patients was carried out by the method of continuous sampling. The inclusion criteria were: patient age of 18-65 years (mean age: 47.1±11.2 years), history of CKD for at least a year, and an ability to understand speech and follow instructions.
The exclusion criteria were: end-stage CKD and receiving renal replacement therapy, presence of a clinically pronounced depressive syndrome, use of medicines that could potentially change the cognitive status (sedatives, tranquilizers, antipsychotics, etc.), as well as the presence of neurodegenerative diseases, potentially leading to CI (Alzheimer’s, Parkinson’s, etc.). In addition, the study excluded patients with CKD who had other factors of non-renal origin recognized by the ESC/EAS clinical guidelines as important in the formation of CVR, specifically: the history of acute coronary syndrome; stable angina pectoris; percutaneous coronary intervention; coronary artery bypass grafting or other operations on the arteries; stroke or transient ischemic attacks; total cholesterol of >8 mmol/L, and/or LDL cholesterol of >4.9 mmol/L, and/or blood pressure ≥180/110 mm Hg; family history of hypercholesterolemia; diabetes mellitus for over 10 years in anamnesis; and the presence of hemodynamically significant atherosclerosis of the cerebral arteries [4].
The examined patients with CKD in the pre-dialysis period were subdivided into three groups, based the criteria for CVR categories proposed by the ESC/EAS Clinical Recommendations (2019) for the correction of dyslipidemia and reduction of CVR in clinical practice (Table 2). Group 1 included 32 patients with a low or moderate CVD and CKD stages C1 or C2 (23 men and 9 women, mean age 40.2±7.8 years); Group 2 comprised 34 patients with a high CVR and CKD stages C3a or C3b (21 men and 13 women, mean age 47.6±11.9 years); Group 3 consisted of 32 patients with a very high CVR and CKD stage C4 (19 men and 13 women, mean age 53.4±10.5 years).
Таble 2. Current categories and criteria of cardiovascular risk (2019 ESC/EAS guidelines for correcting dyslipidemias and reducing cardiovascular risk in clinical practice [4])
|
Risk |
Criteria |
|
Extreme |
|
|
Very high |
|
|
High |
|
|
Moderate |
|
|
Low |
|
ASCVD – atherosclerotic cardiovascular disease; DM – diabetes mellitus; LDL cholesterol – low-density lipoprotein cholesterol; ACS – acute coronary syndrome; PCI – percutaneous coronary intervention; CABG – coronary artery bypass grafting; TIA – transient ischemic attack; CT transient ischemic attack computed tomography; CKD – chronic kidney disease; GFR – glomerular filtration rate; RF(s) – risk factor(s); SCORE – systemic coronary risk evaluation scale; * comments by the authors.
Studied groups were comparable in terms of their gender and age compositions, but their subjects had different duration of the illness, level of GFR decline, and education level. A detailed description of the studied groups is presented in Table 3.
Таble 3. Characterization of study subjects with chronic kidney disease in the pre-dialysis period vs. their cardiovascular risk
|
Indicator |
Group 1 (patients with CKD С1 или С2 and a low or moderate CVR); n=32 |
Group 2 (patients with CKD С3а or С3б and a high CVR); n=34 |
Group 3 (patients with CKD С4 and a very high CVR); n=32 |
|
Age (Me [25%;75%]), years |
40 [32.75; 48.25] |
50.5 [36; 58.75] |
57 [43.75; 64.25] |
|
Gender |
|||
|
Female, abs. (%) |
9 (28) |
13 (38) |
13 (41) |
|
Male, abs. (%) |
23 (72) |
21 (62) |
19 (59) |
|
CKD duration, (Me [25%; 75%]), years |
2 [1; 3.25] |
3 [1; 9] |
6 [3; 10] |
|
GFR, (Me [25%; 75%]), mL/min/1.73m2 |
84 [71.75; 97] |
53 [45; 58.5] |
22 [18.75; 27.25] |
|
Education levels |
|||
|
Higher education, abs. (%) |
30 (94) |
15 (44) |
12 (37.5) |
|
Secondary vocational education, abs. (%) |
2 (6) |
18 (53) |
20 (62.5) |
|
Incomplete secondary education, abs. (%) |
- |
1 (3) |
- |
CKD – chronic kidney disease; GFR – glomerular filtration rate.
All patients underwent clinical and neurological examinations, which included collection of their complaints, anamneses, and a single examination of their neurological and cognitive statuses.
To evaluate cognitive functions, the SAGE test (Self-Administered Gerocognitive Examination) was used, aimed at detecting mild to moderate impairments in memory and thinking. The choice of this test was due to its higher specificity and sensitivity, compared with the more popular MMSE questionnaire (SAGE specificity was 95% vs. 90% in MMSE, and sensitivity was 79% vs. 71% in MMSE), as well as the minimum possibility of a physician’s subjective influence on a patient’s test result, which made it possible to more objectively identify even the initial manifestations of CI in the examined patients [14]. SAGE test consists of 12 tasks on orientation in place and time, objects’ names, finding the similarity among objects, counting, memory, drawing a three-dimensional figure and a clock, assessing the patient’s vocabulary, building a sequence, and transforming a figure. A test result of >20 points was interpreted as normal; the score of 17-19 points implied the presence of a mild CI; 15-16 points suggested the presence of a moderate CI; and fewer than 14 points indicated the dementia.
Our study was approved by the Ethics Committee of the Volga Region Research Medical University and conducted in accordance with the provisions of the Declaration of Helsinki (2013). All examined patients were informed about the study goals and research content, and gave written consent to participate in it.
Data processing and statistical analyses were carried out using MS Excel 2010 software and RStudio integrated development environment. The study groups were compared in a pairwise manner. At the beginning of the analysis, the type of distribution of the studied indicators was determined (the Shapiro-Wilk test was applied). Since the distribution differed from normal, the nonparametric Mann-Whitney test was used to assess the statistical significance of the differences; the median and interquartile range were used to describe the data. Data are presented in the format of the median Me and quartiles [Q1; Q3]. Differences were considered significant at p≤0.05 in the CI study in groups with different education levels. In other cases, multiple comparisons were made (among three groups), hence statistical significance, taking into account the Bonferroni correction, was present at the values of p≤0.017.
Results
According to the results of our study, 27 patients (26.5%) noted a subjective reduction in the concentration of memory and difficulty of thinking. To describe their condition, patients often used descriptors, such as ‘fog in the head’, ‘dullness’, ‘nothing comes to mind’, ‘thoughts are tight’, and mentioned the difficulties in choosing words during a conversation, along with a forgetfulness and difficulties in mastering new skills.
As a result of an objective assessment of the cognitive status via the SAGE test in patients with CKD in the pre-dialysis period, different types of CI were detected at an early stage of the disease. Cognitive dysfunctions progressed with increasing renal failure and the duration of the disease. Accordingly, mild CI was detected in 22.4% (22 patients), moderate CI was revealed in 16.3% (16 patients), and dementia was established in 18.3% (18 patients). Group 1 included 62.5% of patients with no CI whatsoever; in Group 2, there were 55.9% of subjects without CI; in Group 3, only 9.5% of subjects did not have CI (Table 4).
Таble 4. Presence and distribution of cognitive impairment vs. cardiovascular risk of patients and the stage of chronic kidney disease in the pre-dialysis period (according to SAGE test)
|
Indicator |
Group 1 (patients with CKD С1 или С2 and a low or moderate CVR); n=32 |
Group 2 (patients with CKD С3а or С3б and a high CVR); n=34 |
Group 3 (patients with CKD С4 and a very high CVR); n=32 |
|
Subjective signs of CI presence (cognitive complaints), abs. (%) |
4 (12.5) |
9 (26.4) |
14 (43.7) |
|
Objective signs of CI presence (according to neuropsychological testing), abs. (%) |
12 (37.5) |
15 (44.1) |
29 (90.5) |
|
Mean score of SAGE test, Me [25%;75%] |
20.0 [19.0-21.3] |
17.0 [15.0-20.0] |
16.5 [13.8-20.0] |
|
Mild CI, abs. (%) |
8 (25) |
8 (23.5) |
6 (18.7) |
|
Moderate CI, abs. (%) |
3 (9.3) |
4 (11.8) |
9 (28.1) |
|
Dementia, abs. (%) |
1 (3.1) |
3 (8.8) |
14 (43.7) |
|
None, abs. (%) |
20 (62.5) |
19 (55.9) |
3 (9.5) |
CKD – chronic kidney disease; СVR – cardiovascular risk; CI – cognitive impairment; SAGE test – Self-Administered Gerocognitive Examination.
Over half of patients with CKD (53.4%) in the pre-dialysis period, who had CI according to the results of their neuropsychological testing, did not notice subjective disorders and, accordingly, did not complain to the researcher.
The neuropsychological study revealed significant differences in cognitive status in patients with CKD in the pre-dialysis period among different education levels of the respondents. Regardless of the disease duration, dementia was detected less frequently in subjects with higher education than in those with secondary vocational education (p≤0.001).
The greatest difficulties were caused by tasks on counting and short-term memory, the search for similarities between two objects, and construction of a sequence, whereas orientation in space and time, and the function of naming objects remained unchanged in almost all subjects.
In general, in patients with CKD in the pre-dialysis period, we revealed, first of all, impaired memory, along with constructive, spatial and logical thinking disorders. The patients per se most often complained of difficulties in choosing words during a conversation, in mastering new skills, forgetfulness, and ‘tight’ thinking.
The data, obtained in our study, implied the presence of CI in CKD patients already at an early stage of the disease (37.5%). The incidence of CI increased with the progression of a renal failure and the duration of the disease (p≤0.01), and reached 90.5% in Group 3 (patients with CKD C4 and a very high CVR) (Figure).
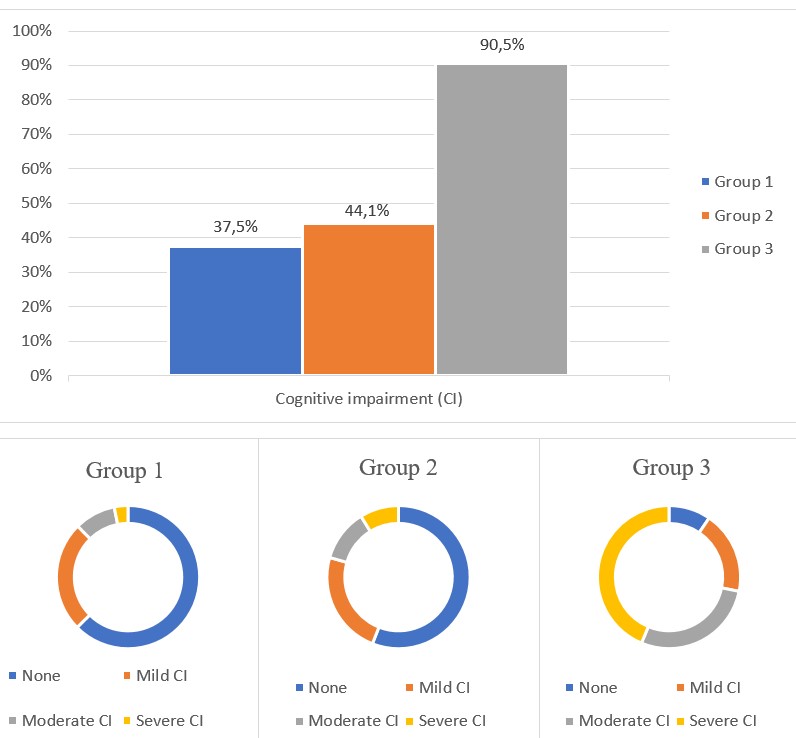
Figure. The incidence and severity of cognitive impairment in patients with chronic kidney disease in pre-dialysis period
Discussion
Our paper describes for the first time the variety and incidence of CI in patients with CKD, depending on the stage of the disease and new criteria for stratification of CVR proposed by ESC/EAS in 2019. According to these criteria, the stage of CKD is one of the factors determining the category of CVR. The study included only patients with factors of cerebrovascular risk, specific for CKD, who did not have other conventional factors of non-renal origin, which fundamentally distinguished our research from a number of previous studies. The CKD stage directly determined the CVR category of examined patients.
The results, obtained during the SAGE test, indicated a high probability of developing CI in this category of patients (in 57% of cases) and a specific role of CKD in the development of CI. Active questioning of patients for the presence of cognitive complaints without supplementary use of cognitive scales and questionnaires turned out to be insufficient and uninformative. Only 26.5% of respondents presented cognitive complaints. Our results suggested the need for timely diagnosis of CI in patients with CKD in the pre-dialysis period, using screening neuropsychological scales (at least once a year). Overall, our data were consistent with the results of another domestic study (Rogova IV et al., 2015), in which CI in patients with pre-dialysis stage CKD were detected in 68.6% of patients [8].
The data on high prevalence of CI in patients with CKD also matched the outcomes of previously performed studies by the foreign authors. For example, in the first systematic review and meta-analysis by T. Etgen et al. (2012), the relationship between the presence of CKD and the development of CI was suggested, and the hypothesis about CKD being an independent somatic risk factor for the development of CD was proposed [12]. As a result of their meta-analysis, the authors concluded that cognitive functions were reduced in patients with CKD, compared with patients without renal pathology (OR 1.65; 95% CI 1.32–2.05; p <0.001) [12]. The likelihood of developing CI in patients with CKD in this meta-analysis was higher in patients with GFR of 45 mL/min /1.73 m2 (CKD stages C3b and C4), compared with patients having GFR <45-60 mL/min /1.73 m2 (CKD stages C2 and C3a), which perfectly matched our data [12].
The results of our study confirmed the hypothesis that CIs could be found already at an early stage of CKD development (CIs in patients with CKD stages C1 and C2 were found in 37.5% of those examined with a low or moderate CVR) and could be expected to progress with increasing renal dysfunction and the duration of the disease (CIs were detected in 44.1% of patients with CKD stages C3a and C3b and a high CVR, and in 90.5% of patients with CKD stage C4 and a very high CVR). All of the above indicates the need for early diagnosing of cerebrovascular and cognitive disorders among patients with CKD in pre-dialysis period, followed by the development of personalized therapeutic strategies.
In our study, in patients with CKD in the pre-dialysis period, memory impairment, along with constructive, spatial and logical thinking disorders prevailed, which was consistent with the data of another previously conducted foreign systematic review and meta-analysis: I. Bergers et al. (2016) noted a wide range of possible CIs in patients with CKD. The authors prioritized the probability of developing the impairments in spatial thinking, attention and speech, separately noting an individual nature of the CI development trajectory in a particular patient with CKD [15].
If CI is detected, further treatment of a patient with CKD should be performed as joint efforts of a nephrologist, neurologist and neuropsychologist, in accordance with the clinical guidelines for CI patient management in the general population. Specific therapeutic approaches to the CI correction in patients with CKD have not been developed as yet. Further research in this field is in a dire need.
Conclusion
Chronic kidney disease is an independent risk factor for the development of cognitive impairment. CI progresses with CKD stage and the patient’s CVR category. CI was detected in 37.5% of patients with CKD and low or moderate CVR, in 44.1% of patients with CKD and high CVR, and in 90.5% of patients with CKD and very high CVR. The results of our study imply the relevance of early diagnosis of cognitive disorders in patients with CKD in the pre-dialysis period, followed by the development of personalized therapeutic strategies.
Conflict of interest: None declared
- Kam-Tao Li P, Garcia-Garcia G, Lui S-F, et al. Kidney health for everyone everywhere: From prevention to detection and equitable access to health care. Therapeutic Archive 2020; 92 (6): 4-14. [In Russ.].https://doi.org/10.26442/00403660.2020.06.000545
- Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease: A systematic review and meta-analysis. PLoS One 2016; 11 (7): e0158765. [In Russ.]. https://doi.org/10.1371/journal.pone.0158765
- Chronic kidney disease: Clinical Guidelines. Association of Russian Nephrologists, 2019. [In Russ.]. URL:http://nonr.ru/wpcontent/uploads/2020/01/Clin_guidlines_CKD_24.11_final-3-3.pdf (12 March 2020)).
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. European Heart Journal 2020; 41 (1): 111-88. https://doi.org/10.1093/eurheartj/ehz455.
- Nikitina AA, Khrulev AE. Cerebrovascular disorders in the pre-dialysis period of chronic kidney disease and the mechanisms of their development. Medical Almanac 2018; 56 (5): 28-32. [In Russ.].
- Khrulev AE, Nikitina AA, Khruleva NS. Specific risk factors for cerebrovascular disorders in patients with chronic kidney disease in the pre-dialysis period. Cardiovascular Therapy and Prevention 2019; 18 (3): 88-93. [In Russ.]. https://doi.org/10.15829/1728-8800-2019-3-88-93
- Polyakova IV, Borovkova NYu, Maslova TI, et al. On the vascular stiffness and cardiovascular risk in patients with chronic glomerulonephritis. Therapy 2019; 28 (2): 89-94. [In Russ.]. https://dx.doi.org/10.18565/therapy.2019.2.89-94
- Rogova IV, Fomin VV, Damulin IV, et al. Vascular cognitive impairments in chronic kidney disease. Neurology, Neuropsychiatry, Psychosomatics 2015; 7 (1): 11-8. [In Russ.]..
- Mark PB. Strategies to manage cardiovascular risk in chronic kidney disease. Nephrology Dialysis Transplantation 2017; 33 (1): 23-5. https://dx.doi.org/10.1093/ndt/gfx329
- Khrulev AE, Studyanikova SF, Langraf SV, et al. Cognitive impairment in patients undergoing programmed hemodialysis. Neurology Bulletin 2019; 51 (2): 36-40. [In Russ.].
- Khrulev AE, Tolbuzova DD, Plokhenko EA, et al. Cognitive status and risk factors for cognitive impairment in dialysis patients. General Intensive Care Medicine 2020; 16 (4): 21-31. [In Russ.]. https://doi.org/10.15360/1813-9779-2020-4-21-31
- Etgen T, Chonchol M, Förstl H, Sander D. Chronic kidney disease and cognitive impairment: A systematic review and meta-analysis. Am J Nephrol 2012; 35 (5): 474-82. https://dx.doi.org/10.1159/000338135
- Matsushita K, Mahmoodi BK, Woodward M, et al. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 2012; 307 (18): 1941-51. https://dx.doi.org/10.1001/jama.2012.3954
- Scharre DW, Chang S-I, Murden RA, et al. A brief cognitive assessment instrument for mild cognitive impairment (MCI) and early dementia. Alzheimer Dis Assoc Disord 2010; (24): 64-71. https://dx.doi.org/10.1097/WAD.0b013e3181b03277
- Berger I, Wu S, Masson P, et al. Cognition in chronic kidney disease: A systematic review and meta-analysis. BMC Med 2016; 14 (206). https://doi.org/10.1186/s12916-016-0745-9